AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2768-0487/024
1Department of Pediatrics, General Pediatrics Unit, MD, Ege University Faculty of Medicine, Ege University, Bornova, 35040, Izmir, Turkey.
2Associated Professor Doctor, Department of Pediatrics, General Pediatrics Unit. Associated Professor Doctor, Ege University Faculty of Medicine, Ege University, Bornova, 35040, Izmir, Turkey.
*Corresponding Author: Şule Gökçe, Department of Pediatrics, General Pediatrics Unit, Ege University Faculty of Medicine, Ege University, Bornova, 35040, Izmir, Turkey.
Citation: Ş Gökçe, A Aslan, F Koç. (2021) Malnutrition: Already exist and is being overlooked?. Journal of Clinical and Laboratory Research. 2(5); DOI:10.31579/2768-0487/024
Copyright: ©2021 Şule Gökçe. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 May 2021 | Accepted: 14 May 2021 | Published: 26 May 2021
Keywords: malnutrition; pediatric patients; nutritional status; anthropometric measurements
Background: Malnutrition is defined as deficiency and or imbalance of nutrients and energy and may produce a negative effect on the growth, maintenance, and specific functions of the body. This study purposed to determine the nutritional situation, to define the presence of malnutrition, to detect the deficiencies of micronutrients of the children admitted to a pediatric tertiary hospital.
Methods: A retrospective, cross‑sectional, single unit-based study in pediatric patients admitted to the pediatric wards for differential diagnosis or treatment was conducted between November 2017 and December 2019. The anthropometric measurements were figured out on hospital admission of all pediatric patients. The pediatric patients diagnosed with malnutrition were assessed to detect their nutritional status/feeding habits and to identify any associated factors.
Results: A total of 1206 children were hospitalized with an acute illness diagnosis and/or treatment during the study period. One hundred fifteen patients were noted to have malnutrition; acute malnutrition (wasting) (weight for height z-score < - 2 SDS) (n=51/115, 44.3%) and chronic malnutrition (stunted) (height-for-age < −2 SDS) was detected in 64/115 (55.7%) patients; the prevalence of wasting, and stunting was 4.2% and 5.3%, respectively.
Conclusions: Our study suggests that it should be performed an assessment of nutritional status/ history and anthropometric measurements every admission to the hospital in order to provide healthy growth development in childhood, particularly under 2 of age and interventions should be strengthened for general child health.
Malnutrition is a clinicopathological entity that characterized a deficiency, excess, or imbalance of nutrients, occurs predominantly in children under five years old in particularly low-income and middle-income countries. According to data from the World Health Organization (WHO), there are 52 million wasted children under 5 years of age, 17 million severely wasted children, and 155 million stunted children in the world. It is known that around 45% of deaths among children under 5 years of age are associated with undernutrition in low- and middle-income countries [1]. A total of 1.300 children < 5 years of age were noted to be in an increased risk of death related to all types of undernutrition (stunting, wasting, and underweight) in ten longitudinal studies including ~54,000 child-years of follow-up [2]. Data from the Turkey Demographic and Health Survey in 2018 revealed the prevalence of acute malnutrition [weight for age <− 2 standard deviations (SDS)] in 17.9% and chronic malnutrition (height-for-age <− 2 SDS) in 6.9% of children aged ≤ 18 years in the general population [3]. An important condition together with malnutrition is also micronutrients deficiency that defines a lack of zinc, iodine, iron, selenium, copper, vitamins A, E, C, D, B2, B6, B12, and folic acid. Today, more than 2 billion people in the world suffer from malnutrition of micronutrients (collectively referred to as essential vitamins and minerals) that play a conductor role in the production of enzymes, hormones, and other substances and to be regulatory for growth activity, cognitive development, and functioning. Due to their major tasks, they should think to be as a blocking element the childhood morbidity and mortality [4, 5]. Micronutrients including iodine, vitamin A and iron intake under five years old children have been insufficient in 122 countries according to the WHO data. Most of the nutrition problems together with poverty and poor socioeconomic status in children result from their inability to supply the micronutrient requirements [6].
Several studies have shown that undernutrition has been an important problem primarily of hospitalized children with a declared prevalence of 5% in developed countries and up to 50% in developing countries [2]. Generally, the prevalence of undernutrition in hospitalized children has been reported with a range of 6%-30%; from 6% to 14% in Germany, France, UK, and the USA [7, 8]. The rates of malnutrition have been previously reported in our country as 31.8 to 56.6% in hospitalized pediatric patients [9].
There is no consensus for an optimum method of assessing the nutritional risk of children admitted to the hospital; however, the nutritional screening tools help to raise the clinician’s awareness of nutritional risks and to detect early diagnosis of malnutrition, ideally on every admission to the hospital [10]. The evaluation of the nutritional risk of the pediatric patient via the most recent instruments known Screening Tool for Risk on Nutritional status and Growth (STRONGKids) tool is a comprehensive summary of commonly asked questions concerning nutritional issues and a clinical view of the child’s status.
In the light of this informations, the aim of this study was to evaluate pediatric patients’ nutritional status at the moment of their hospitalization in a pediatric hospital, to ascertain nutritional risk by application of the STRONGKids, to elucidate demographic, socio-economic factors associated with malnutrition and to define the deficient micronutrients in hospitalized children.
Study Setting and Design
We performed a retrospective, cross‑sectional, a single unit-based study in pediatric patients admitted to the pediatric wards for differential diagnosis or treatment, Ege University, Children’s Hospital, a 200 bed, tertiary-care facility in İzmir, from November 2017 to December 2019. The children with malnutrition were enrolled in the study. Approval for the study was granted by the Local Clinical Research Ethics Committee of Ege University (99166796-050.06.04/20-6.1T/72).
Patients
A total of 1206 pediatric subjects were hospitalized consecutively in the Pediatric Hospital of Ege University of Medical Sciences for differential diagnosis/diagnosis and treatment from November 2017 to December 2019. When all patients were evaluated, 115 pediatric patients diagnosed with malnutrition (1 month–18 years of age) were included in the study. Patients with overweight and obesity, neurological sequelae, newborns, and those admitted to an emergency, neonatal intensive care, and the intensive care unit were not included in the study as there may have been associate factors with malnutrition. Those with recurrent hospitalizations or hospitalization of less than 24 h were also excluded. After application of exclusion criteria, the interview was undertaken with the parent or caregiver who had been with the patient for most of the time during the previous 48 h. The malnourished 115 children (aged 1 month to 18 years; of both genders) were screened by examination of detailed medical records, and physical examination.
A uniform questionnaire was administered to the parent or caregiver who had been with the patient for most of the time during the previous 48 h. Informed consent was obtained from the caretaker prior to undertaking the interview by trained medical personnel (health officers). The questionnaire comprised the following parts: demographic characteristics, health status, and diet factors. The following information regarding health status was collected during the interview: fever in the last 15 days and weight loss.
Within the first day of admittance to the General Pediatric Unit, measurements were taken of body weight, height, mid-upper arm circumference (MUAC), and triceps skinfold thickness (TSF). Body mass index (BMI) was calculated in all children over two years of age. Under-nutrition was defined according to WHO criteria. Malnutrition; together with demographic characteristics, health status, and nutrition factors was evaluated in the subjects. Socio-demographic and economic related determinants like maternal age, maternal religion, parents education, maternal occupation, family size, number of under-five children, sex, child age, maternal and child health care characteristics were also assessed in the index study.
The patients were separated into groups according to diagnosis as infection, gastrointestinal, endocrine, genitourinary, collagen tissue, chronic respiratory system, malignancy, and non-malignant hematological diseases and others. Peripheral blood samples were obtained from all patients for blood count and biochemical measures of micronutrients, and other biomarkers of nutrition. The nutritional assessment consisted of the following features: Biochemical analysis, including glucose, pre-albumin, albumin, total lymphocytes, total cholesterol, triglycerides, and the serum ferritin test. The hematological assessment included a complete blood cell count [hemoglobin level, hematocrit, mean corpuscular volume, and mean corpuscular hemoglobin concentration, red blood cell (RBC)], serum ferritin, vitamin B12, folate, and albumin. Anemia was defined as a hemoglobin level of ≤11.5 g/dL. A value <13 indicates thalassemia trait and >13 indicates iron deficiency. A structured proforma for data collection was developed with input and contribution from all investigators. Categories and criteria were defined to ensure uniformity in data collection. All investigators were assessed regarding their understanding of the methods and all were trained in the correct ways to measure heights and weights. Subsequently, the STRONGKids tests were applied, according to anthropometric measurements.
The primary outcome was to determine the prevalence of malnutrition with respect to anthropometric measurements. The secondary outcome was to determine the status of daily intake/micronutrient/vitamin of the patients and to detect whether there was a difference between acute and chronic malnutrition in the nutritional intakes.
Definition of Malnutrition
Pediatric patients aged below 2 years were weighed unclothed on a 16 kg capacity baby scale with 10 g sensitivity (Seca 334, Hamburg, Germany) and aged over 2 years were weighed on an adult scale with 100 g sensitivity (Seca 769, Germany). The height of children aged below 2 years was measured with a 1 m measurement scale of 0.1 cm sensitivity, with the child supine on a flat surface, the head held still, and the feet together. Those aged over 2 years were measured standing upright with a fixed measurement scale of 0.2 cm sensitivity. Mid-upper arm circumference was assessed with a non-elastic measuring tape with 1 mm gradations, with the left elbow joint in mild flexion from the acromion notch to the center of the olecranon notch. Skinfold thickness was measured at two sites (tricipital and subscapular) to the nearest 0.2 mm using a Holtain caliper (Holtain Ltd., Crymch, SA41 3UF, UK) [11]. Malnutrition was evaluated based on anthropometric measurements ((weight, length/height, MUAC, TSF that were performed by the same ward staff. For acute malnutrition, Weight-for-Height (WFH) SD ≥-3 to <-2 were considered moderate malnutrition, and <-3 SD as severe malnutrition. For chronic malnutrition, Height-for-Age (HFA) <-2 SD were named chronic malnutrition in accordance with WHO classification. Mid-upper arm circumference Z scores were calculated for patients aged ≤60 months only, in compliance with WHO standards.
• WFH = [observed weight/median height (same height and sex)] × 100.
• HFA = [observed height/median height (same age and sex)] × 100; [12].
Nutritional risk screening tool Screening Tool for Risk on Nutritional status and Growth (STRONGKids)
The risk for malnutrition was evaluated via the STRONGKids questionnaire, which was completed by physicians via the face to face method. STRONGKids is a malnutrition “risk assessment tool” that consists of 4 items (Supplementary file). The first 2 items were assessed by a pediatrician and the second 2 items were discussed with the parents or caregivers. Questions answered with ‘unclear’ were classified as ‘no’. Patients with STRONGKids score 0 were classified as “low risk”, whereas those with a score of 1–3 were classified as “medium risk” and those with a score of 4–5 were classified as “high risk” [13].
Socio-economic status
The socio-economic index for areas was calculated for all patients using their postal code as recorded at admission. This area-based approach is inexpensive, objective and the required information is readily accessible. A low index value reflects relative disadvantage and occurs where there is a large proportion of low-income families, people with low skilled occupations, and high proportions of the population without training, whilst a high value reflects a lack of disadvantage in an area. According to these index values, Izmir city is one of the most developed provinces in Turkey [14].
Dietary intake
Dietary intake data were collected using a uniform questionnaire that was administered to the parent or caregiver who had been with the patient for most of the time during the previous 48 h. Portion sizes were estimated using measuring cups and spoons. Pictorial food models of commonly eaten foods were also used to closely estimate the amount consumed. Micronutrient intakes were compared to Estimated Average Requirement and Recommended Nutrient Intake to evaluate nutrient adequacy according to age and sex.
The statistical analyses
The statistical analyses of the study were made using the Statistical Package for the Social Science for Windows (SPSS) v. 21.0 statistics program (SPSS Inc, Chicago, IL, USA, 2006). By calculating the mean and standard deviation values for the distribution of measurable variables, a comparison of the grouped data with defined numbers was made with the Chi-square test, and a comparison of the mean values of the measurements of the independent two groups was made using the Mann–Whitney U test. The Pearson correlation was used to analyze the statistical relationship between demographic and laboratory parameters. A value of p<0.05 was accepted as statistically significant for all results.
Patient demographics and basic clinical features
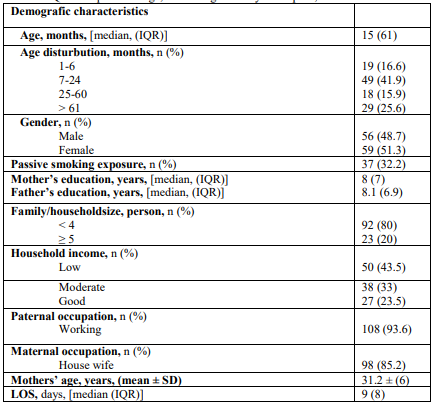
During the study period, in total 1206 children were considered for enrollment and hospitalized for diagnosis or/differential diagnosis and for treatment in the medical ward of Ege Childrens’ Hospital. To evaluate the nutritional status of the patients; WFH and HFA and were calculated and the final study population comprised 115 children with malnutrition fulfilled the study criteria and completed the evaluation. The demographic and socio-economic features have been shown in Table 1. The prevalence of acute and chronic malnutrition was 9.5% over the study period. The patients included 56 (48.7%) males and 59 (51.3%) females with a median age of 15 (61) months (range, 1 month–18 years). Sixty-eight patients (59.1%) were aged less than 2 years of age. The highest percentage of children (52.6%) in the undernourished group were aged <60 months. In the 7-12 months group, 60.4% of children were either moderate or severe malnutrition, whereas none in >60 months age group was deteceted as severe malnutrition.
"Prevalence of undernutrition/Anthropometric measuraments results//Medical Diagnosis"
Upon admission, the prevalence rates of acute and chronic malnutrition were 95/1000. According to the WHO criteria, 51 (44.3%) patients were wasting, and 64 patients (55.7%) were stunted. Severe malnutrition has been detected in 18 (15.7%) patients of the children diagnosed with wasting (Table 2). The medical diagnoses leading to hospitalization have also shown in Table 2. Approximately one-third of (38.3%) of the patients had an underlying chronic medical illness. Two major groups of medical conditions leading to hospitalizations were acute infectious diseases and respiratory/gastrointestinal disorders followed by neurologic and cardiovascular diseases.

STRONGKids risk classifications
When the patients were evaluated with the nutritional risk scoring system-STRONGKids-, high risk was found in 26 (22.6%) patients; 79 (68.6%) of the children were classified as having medium risk, and the low risk was found in 10 (8.6%) patients. For all patients hospitalized with any disease or diseases, the median STRONGKids score was 2 (2) in the malnutrition accompaniment group compared to the groups with and without malnutrition accompaniment system, whereas in the malnutrition accompaniment group, this score was 0 and was statistically significant (p < 0.001). Thirty-three (28.7%) of children had chronic disease; the children (n=21; 11 [52.3%]) with neurological disorders and 8 patients (38%) with respiratory problems had high risk for nutrition. The STRONGKids results indicated that the proportion of the high malnutrition risk patients with an underlying chronic disease was higher than the patients with a medium or low risk (91% compared with 47% or 45%, respectively). There was a significant negative correlation between the z score of weight for height and STRONGKids z scores (p < 0.001, r=-0.3) in malnutrition patients. With regard to STRONGKids risk scores, there were no differences in the gender distribution, mean age in months, and age categories between the high and low nutritional risk group (data not shown).
Risk factors for undernutrition
Various sociodemographic factors were analyzed to determine the risk factors leading to undernutrition in children requiring hospital care. There were no associations between risk factors and malnutrition via univariate analysis. In addition, children with severe malnutrition were more likely to have a lower quality of life, and a more frequent occurrence of gastrointestinal disorders (data not shown).
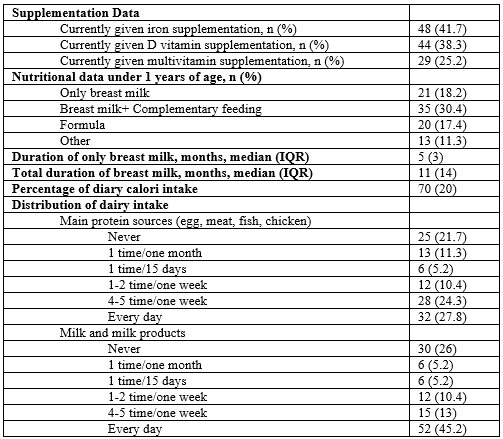
Dietary intake and suplementations
The nutritional data, supplementations, and dietary intake have been summarized in Table 3. As shown in Table 3, macro protein intake has been found insufficient in 44 (38.2%) patients. Even, 21.7% of the 115 patients can not reach the source of macro protein sources.
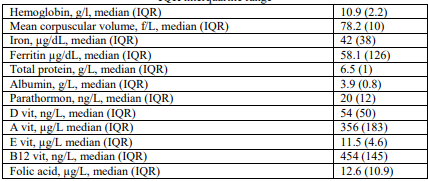
Laboratory data
The levels of the blood parameters of the children were detailed in Table 4. Iron deficiency and anemia were identified as the most important factors leading to micronutrient malnutrition The lower prevalence of anemia among the children may be due to national programs implemented by the Ministry of Health, such as the Programme on the Iron supplementation. Under this program, food baskets containing essential food items, as well as Fe, D vitamin, and multivitamin supplements, are distributed to eligible recipients on a monthly basis. Family Health Clinics also routinely disseminate nutrition education.
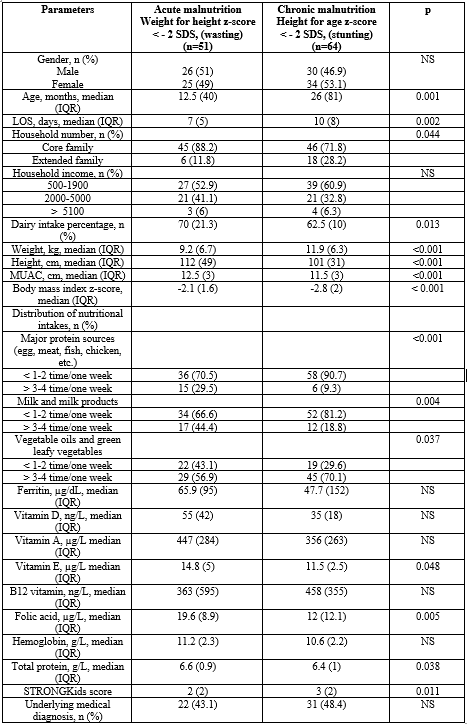
Comparison of anthropometric measurements at the hospital admission with patient characteristics
There were no gender differences in the wasting/stunting group. At the time of admission, 55.7% of the participants had an HFA standard deviation score of less than −2. Children with chronic malnutrition were older than those with acute malnutrition. A total of 32.8% of patients with acute malnutrition were younger than 24 months of age. Patients with low-income levels and a high number of siblings were noted to have high in the chronic malnutrition group. The underlying chronic disease prevalence rates were not found statistically between the groups. The length of stay in hospital was significantly higher (p < 0.002) in patients with HFA SD < -2. There was a high prevalence of vitamin E and folic acid deficiency in chronic malnourished children compared with patients with acute malnutrition.
This current study has revealed again that malnutrition is still an annoyance for children that should be assessed an accurate and adequate nutritional in the clinical management to be ensured their normal growth and development in a having high socio-economic index values city. It is essential that the evaluation of the nutritional status of children for being a healthy person and to prevent the adverse interactions between nutritional status and the patient’s medical condition in any admission to the hospital. Our study purposed to define the nutritional conditions of the patients via anthropometric measurements at hospital admission and to define the related concomitant factors. SD −2 or less for WFH and HFA were indicators of acute and chronic malnutrition, respectively [10]. We found the acute and chronic malnutrition rate to be 9.5%. Previous small-scale and local studies performed in Turkey found higher acute and chronic malnutrition rates (31.8% and 27.7%), respectively, when weight for height parameter was used and the cutoff value is accepted as −2 [15, 16]. We believe that the primary reason for reported lower rates was related to the number of undernutrition patients for assessing the nutritional status of the patients. Most of the patients do not need to be hospitalized for undernutrition, therefore our rate was lower than the several studies. In addition, there is significant variability in the declared incidence of malnutrition due to differences in patient populations, and the method or nutritional marker used for diagnosis. During the hospitalization, it is essential that the detection of the patients' nutritional status and anthropometric measurements that can provide the correction of nutritional behavior, improve the patient’s prognosis, and shorten the length of hospitalization soon after admission. Supplying balanced nutrition and adequate micronutrients is an important effective factor for continuous growth and development that occur throughout the childhood period and it provides to avoid mortality and morbidity associated with malnutrition.
As in previous studies, most of the patients were younger than 2 y of age in the study [17, 18]. The children with chronic malnutrition were older than those acute malnutrition; and it was found that they had a longer length of stay hospitalization, with a higher rate of STRONGKids scores. In our study, we also found that the patients with chronic malnutrition at hospital admission could not reach the main protein sources and dairy intake percentage was low than those of acute malnutrition. Additionally, the patient with chronic malnutrition at hospital admission had a crowded family.
It has been known that the prevalence of acute and chronic malnutrition of children admitted to the hospital since the 1980s, particularly in developing countries [19]. Black RE, et al. stated a study - is an important global review of the epidemiology, major risk factors, and consequences of malnutrition 875,000 deaths were related to wasting that cause of death of 12.6% of children <5 years of age and 516,000 deaths were attributable to severe wasting that cause of death of 7.4% of children <5 years of age [20].
The prevalence of malnutrition was reported from 10% to 50% in children under the age of five in our country [15, 16]. Data from the Turkey Demographic and Health Survey in 2018 revealed the prevalence of acute malnutrition (weight for age <-2 SD) in 17.9% and chronic malnutrition (height-for-age <-2 SD) in 6.9% of children aged ≤18 years in the general population. In the index study, the prevalence rate of malnutrition has found in 95/1000 pediatric patients in inpatient clinics. The study has not included outpatient groups.
Today, the malnutrition has been separated to three main types that called undernutrition [wasting (low weight-for-height), stunting (low height-for-age) and underweight (low weight-for-age)]; micronutrient-related malnutrition (a lack of important vitamins and minerals) or micronutrient excess; an overweight, obesity and diet-related non-communicable diseases (such as heart disease, stroke, diabetes, and some cancers) [21-23]. Micronutrient-related malnutrition could be an occasion for morbidity and mortality in children. Based on the prevalence of the vitamin deficiencies in both groups of acute and chronic malnourished children, there is a need for all pediatric patients that present to hospitals and clinics to be assessed for this nutrient. Unexpectedly, there were no statistically significant differences and deficiencies in the vitamin status for the two groups in this study. With regard to D vitamin, the deficiency is likely to be highly prevalent among children presenting to hospitals in this region that is rich with sunshine all year round, due to the possibility of under-reporting or under diagnosing. Deficiencies of folic acid and vitamin B12 are often part of general malnutrition. Folic acid, also known as folate and vitamin B9, is a water-soluble vitamin that must be obtained either through the diet or from supplementation. [24]. Its absence leads to megaloblastic anemia, and it has also been determined that the nutritional status of folic acid may be associated with chronic diseases and information dysfunctions. Despite other micronutrient levels, folic acid was found to be low in patients with chronic malnutrition compared to patients with acute malnutrition. It could be explained with an inadequate intake of pulses and pulses products for our cohort. Major dietary sources of E vitamin are vegetable oils, nuts, whole grains, and green leafy vegetables. According to the Food and Nutrition Board of the Institute of Medicine, vitamin E deficiency in normal is defined by a plasma α-tocopherol concentration < 12 μmol/L (0.5 mg/dL) based on the association of greater concentrations [25]. The primary manifestations of prolonged vitamin E deficiency include spinocerebellar ataxia, skeletal myopathy, and retinopathy. Similarly, our chronic malnourished patients had lower vitamin E levels than acute malnourished subjects; however, no study patients manifested the neurological deficits associated with deficiency of Vitamin E. Multivitamin preparations are generally given by general practitioner for patients with underweight; it could be explained with normal reference levels of other micronutrients and vitamins in these children. In order to reduce or prevent the malnutrition that may cause mental and motor disabilities complications in children in developing countries, European Society Clinical Nutrition and metabolism has suggested early identification of nutritional status in children should be considered during the hospitalization for any diagnosis [26].
In conclusion, in the present-days, to control the COVID-19 pandemic, it could be a high probability of neglected and/or overlooked the diagnosis of several diseases (malignancies, obesity, etc.) and malnutrition due to the several strategies. Healthy living is defined as a state of good health in physical, mental, spiritual, and social aspects, and directly affects maintaining a healthy life. When adequate and balanced amounts of each of the essential nutrients are available, the children may be protected from several nutrition problems such as protein-energy deficiency, iron deficiency anemia, iodine deficiency disorders, rickets, tooth decay, obesity, etc. Therefore, the establishment of healthy nutrition policies, the evaluation of the nutritional status of each patient should be made a habit and considered as part of the examination.
BMI = Body mass index
COVID-19 = Corona Virüs Disease 2019
HFA = Height-for-Age
MUAC = Mid-Upper Arm Circumference WHO = World Health Organization
SD = Standard Deviation
SPSS = Statistical Package for Social Science
STRONGKids = Screening Tool for Risk on Nutritional status and Growth
TSF = Triceps Skinfold Thickness
WFH = Weight-for-Height
The authors would like to thank Prof. Dr. Sadık Akşit who died on March 2020 and staff of the General Pediatrics Unit and the parents of the children to participate the study.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
The datasets analyzed during the current study are available from the corresponding author upon reasonable request.
ŞG, AA, and FK conceived and designed the study, performed analysis, interpreted the data. ŞG prepared the manuscript, and all authors read and approved the final manuscript.
The study was approved by the institutional review board named The Ethics Committee of Ege University (99166796-050.06.04/20-6.1T/72).
This manuscript does not report personal data such as individual details, images, or videos; therefore, consent for publication is not necessary.
The authors declare that they have no competing interests.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
